Research Assistant Professor Monir Shababi and mothers of SMARD children started out as friends on Facebook. Now, they’re friends for a lifetime.
It was an unexpected turn for someone who spends most of her professional life in a lab.
SMARD1 is an acronym for the rare genetic neuromuscular disease spinal muscular atrophy with respiratory distress, which has been the focus of Shababi’s research for the past five years. While it shares part of its name with the better known spinal muscular atrophy (SMA), the disease-causing gene is not the same. Both diseases target the lumbar motor neurons and cause muscle atrophy, diaphragmatic paralysis and respiratory complications are the first and most devastating symptom of SMARD.
“When my first paper about gene therapy for SMARD1 disease was published, a mother of the SMARD child contacted me and she informed other moms about my research,” Shababi said. “I never thought it would happen this way, you never imagine there would be a personal impact with your publications.”
Shababi ran into the obstacle of funding. Her once Facebook friends were there to help Shababi face this drawback.
“Within the second year of my National Institute of Health funding for SMARD1 gene therapy, I discussed the research with the mothers of SMARD kids, Jill Sims and Lisa Porter,” Shababi said. “I told them about the limited funding options in the future. Sims and Porter family were extremely supportive and generous. Dr. Sims and his wife (Jill’s in-laws) donated a large sum of money to Mizzou Give Direct, MU’s crowdfunding website exclusively for my SMARD research, establishing a webpage for donations with the goal of curing SMARD. Their gift changed the course of many lives in the most meaningful way.”
Shababi met the Sims daughter Catherine a few weeks ago. Catherine is five years old and lives with the disease.
“It had the most amazing personal impact on my work, which I was looking all along in my professional life,” Shababi said. “This is not just a job, it is not just research, it is not about publishing papers; it is affecting real lives.”
Shababi — who works with Dr. Chris Lorson at Bond LSC — began her life career in science at the University of Tabriz in Iran studying plant pathology. She moved to America with her husband, who accepted a research job in MU. She then got her masters and Ph.D. through the university, finishing her Ph.D. in Dr. James Schoelz lab studying gene regulation in a plant virus. She then had two postdoctoral positions working on gene regulation in yeast and bacteria.
“My postdoc research on yeast and bacteria was not satisfying enough; I wasn’t feeling the impact on the society that I was looking for,” Shababi said. “I even thought about changing careers until I contacted Dr. Lorson. His research involved hereditary genetic disease in humans and using virus as viral vectors to deliver the missing gene. I thought this research will surely have an impact on human lives. In Lorson’s lab, I found the enthusiasm and passion which led to four funded grants, 18 publications, a book chapter and most importantly, a financial gift to MU.”
Even if Shababi doesn’t get the expected results, every day in the lab is a new victory for her. She has developed a new mouse model for SMARD1 and injects them with the therapeutic virus at different times with different dosages to determine the therapeutic window and proper dosing for the vector. Shababi previously tested only black mice but now tests new white mice born with SMARD.
“As opposed to black mice, these white SMARD mice do not have the genetic modifiers to survive for a long period of time,” Shababi said. “They usually die by day 20, so we administer the gene replacement therapy at different days post birth or different dose and analyze the survival and overall health. Even a few days elongated survival is a huge improvement and you can tell if that time point or dose was still efficient or not.”
To move the research further toward clinical trials, the lab aims to use a more advanced model such as a human primate.
“We are hoping to advance from the mice research to an animal closer to humans,” Shababi said.
With hopeful new advancements in the future, there is only a positive outlook for the future of treatment.
“The pain and suffering of SMARD children and their parents are real and heartbreaking,” Shababi said. “This research builds a foundation for the future clinical trials creating optimism and hope for the SMARD community.”
For scientists, studying a disease presents a puzzle looking for an answer, but there are real people behind the research that may one day cure the illnesses that turned their lives upside down. Chris Lorson and Monir Shababi work on one of these puzzles in Bond LSC.
Find out more about their work and the faces behind SMARD, a rare, often fatal, genetic motor neuron disease in the following story courtesy of the College of Veterinary Medicine.
Monir Shababi, an assistant research professor in veterinary pathobiology, and Christian Lorson, Bond LSC principal investigator, College of Veterinary Medicine professor and associate dean for research and graduate studies, have invested countless hours during the past five years to solving a cruel medical mystery. A family who has endured the agonizing ordeal of having two children born with the same disease has invested funding for the research being conducted at MU’s Bond Life Sciences Center.
Meet the Sims family: mother, Jill Sims, MD; daughter, Caroline; father, Eric, an associate professor of economics at Notre Dame; daughter, Molly; and daughter, Catherine, who turned 5 in August. Catherine is living with a rare genetic disorder called Spinal Muscular Atrophy with Respiratory Distress, or SMARD. The Sims had another child, Bobby, who was born in 2012 and died of SMARD after a month of life.
The disease is called spinal muscle atrophy with respiratory distress, or SMARD. SMARD is a progressive motor neuron disease that has no treatment or cure. At least, not yet.
Shababi, PhD, and Lorson, PhD, and the Sims family — mother Jill, father Eric, grandparents Grant and Patricia — have teamed up in an effort to change that.
*****
The disease is so rare that it is largely unknown, even to most medical professionals. When you are the parent of a child with SMARD, you are in a daily, nonstop, life-and-death struggle.
It is exhausting. It is frustrating. It is a battle that requires an endless reserve of endurance and willpower. And, it requires cutting-edge, scientific discoveries that are just coming to light at MU’s Bond Life Sciences Center.
*****
Catherine Sims lives on a ventilator and needs around-the-clock care. Yet, now age 5, her life is a victory.
“Our first daughter was born healthy, so we had no idea that we carried such a terrible disease,” Jill Sims says. “Then, our second child, Bobby, — who is named after my dad — was born very small, which was unusual given our family history, and he was very quiet as an infant. Those were the only things I noticed. He was three weeks old and we were driving back from Thanksgiving at my parents’ house. I fed him and put him in his car seat. I checked on him 30 minutes later and he had died. He had aspirated. The disease causes the diaphragm not to work, so he couldn’t breathe and eat at the same time.”
Despite requiring mechanical ventilation and around-the-clock care, Catherine attends school, enjoys family outings and participates in activities as much as possible.
Bobby Sims, born Oct. 31, 2012, died on Nov. 30, 2012. His death was attributed to unknown respiratory failure, and he was considered a victim of Sudden Infant Death Syndrome (SIDS). Catherine Sims was born in August 2013; her diagnosis came four months later.
“I went on to have Catherine next, and then we knew something was up,” Sims says. “Catherine was very similar to Bobby, very small and very quiet. That, of course, led us to figure out something was going on.
“In the period of time when Catherine was having problems and was hospitalized but undiagnosed, Catherine had a test done that put her group of symptoms into a specific category of neuromuscular diseases,” Sims says. “A good friend of mine Googled that category and the search produced a WordPress blog that Lisa Porter Werner had contributed to.”
The blog contained personal stories of families who had children with a disease named SMARD. The goal of the blog was to put SMARD on the radar, for families who didn’t have a diagnosis and needed to find answers as well as find support. Porter Werner had posted her own family’s story.
“My friend forwarded me Lisa’s particular story regarding her two children with SMARD, and the story almost identically matched my own,” Sims recalls.
Porter had read extensively and combed the internet for information and cases similar to those of her children. Porter eventually found a modicum of information about something called SMARD, which had been diagnosed in approximately 60 children.
“Lisa Porter’s blog contained the personal stories of families who had children with SMARD,” Sims recalls. “My friend forwarded me Lisa’s particular story regarding her two children with SMARD, and the story almost identically matched my own.
Living with SMARD, a progressive motor neuron disease, means Catherine needs 24/7 care from her family and home-health attendants.
“The Werner’s first daughter died at six weeks of age. It was called a SIDS case; she just died in her sleep,” Sims says. “They had Silas, their son who is living with SMARD, shortly thereafter and she put him in a sleep study when he was three weeks old. She said, ‘No, my daughter didn’t just die. There was a reason.’ It turned out that Silas was having major breathing problems during sleep.
“I was convinced after reading about Lisa’s family that my two children had SMARD as well, and I asked Catherine’s doctors to test her for it,” Sims says. “Catherine’s test came back positive four weeks later. A year or so later, I connected with Lisa through a Facebook group for families with children with SMARD. We began talking more, once my in-laws funded SMARD research at the Jackson Lab, and continued to talk once we found out about Dr. Shababi’s paper that came out in 2016.”
*****
In order to know what SMARD is, it is important to know what it is not. Despite the obvious similarities in name, spinal muscular atrophy (SMA) and spinal muscular atrophy with respiratory distress have sharp differences.
Both conditions affect the lower motor neuron cells of the spinal cord that control voluntary muscle activities like walking, talking, breathing and swallowing. Both are sometimes characterized as “like ALS in babies.”
SMA, which can range from type 1-4, is caused by mutations in or the absence of the SMN1 gene. SMA typically causes weakness in the core first and the baby or child may present as hypotonic, or having low muscle tone — sometimes called floppy baby syndrome. Babies or children with SMA may eventually develop respiratory compromise over time.
SMA is the leading genetic killer of infants; one in 40 people are carriers of SMA.
SMARD, in contrast, is extremely rare. The exact number of cases is unknown, but it has clearly occurred in more than the approximately 100 children worldwide who now carry that tragic diagnosis. SMARD is branded an “orphan” disease, a term commonly applied to any debilitating medical condition that affects fewer than 200,000 Americans. There is little information and few resources available regarding SMARD.
The Sims sisters: Catherine, a SMARD survivor, with older sister Molly and younger sister Caroline. Catherine is standing with the aid of a device.
SMARD is a genetic disease, caused by mutations or loss of the IGHMBP2 gene, Immunoglobulin MU-binding protein 2. The condition is inherited in a recessive pattern, meaning both parents must be carriers of the gene mutation and each parent must pass along a copy of the mutation in order for the child to be affected. In essence, every time two carriers have a baby, there is a one in four chance their child will be affected.
Onset of the disease usually occurs suddenly, in what seems to be an otherwise healthy baby, typically between 6 weeks and 6 months of age. Once the diaphragm is paralyzed, the infant must depend on their accessory muscles to breathe. These muscles also weaken as the disease progresses, until the child needs mechanical ventilation.
Many children die in the first year of life, often in their sleep or from a respiratory illness. Past the age of 1 year, almost all children living with SMARD require a tracheostomy, a ventilator and a wheelchair.
Simply put, SMA usually presents as a hypotonic or “floppy” baby who gradually develops respiratory distress. SMARD presents as a baby in respiratory distress who gradually becomes hypotonic.
SMA and SMARD share a similarity in that both are monogenic disorders, conditions caused by mutations or loss of a single gene. Shababi and Lorson have an established history of working with SMA. Now, their focus is SMARD.
*****
“In 2009 and 2010, a lab at the Ohio State University used a viral vector to introduce the SMN gene in SMA mice,” Shababi, the CVM researcher, says. “The viral vector does not contain the necessary genes required for the virus to cause infectious disease. You can replace viral genes with the specific gene you want and keep only the part of the virus that is required to enter the body, find its receptor and produce the desired protein from the gene it carries.
“They (researchers at Ohio State) put a human SMN gene into a viral vector — adeno-associated virus 9 (AAV9) — that has the potential to pass the blood brain barrier in humans. This virus has the capability to enter into the brain, the spinal cord, muscles and peripheral organs,” Shababi continues. “The AAV9 virus carrying the SMN gene was injected into SMA mice. They were able to rescue the affected mice. That was a huge step toward treating SMA. That vector is currently in Phase 2 clinical trials with AveXis/Novartis.
“With SMARD, there is also a single gene involved in the disease — the IGHMBP2 gene,” Shababi continues. “So, we took a human IGHMBP2 gene, in the form of cDNA, and placed it into the same AAV9 vector and injected it into the brain of SMARD pups that were 2 days of age. Our virus did the job and the SMARD mice were cured.”
*****
Catherine and older sister Molly sporting festival face paint.
“Dr. Shababi posted a paper, I believe in March 2016, that reported the results of her work on SMARD,” Sims says. “Lisa found the paper and contacted Dr. Shababi and had a wonderful reception. They had several very long conversations about what Monir was doing, what she had already been doing, and they immediately had a strong connection.
“Dr. Shababi was very personable over the phone, and was very passionate and very approachable about her work,” Sims relates. “Sometimes, it’s hard to get ahold of people, but Monir answers her own phone, and she was very clear with Lisa about what had already been done, which was pretty cool for us because we didn’t know — we didn’t realize how much work Dr. Shababi and Dr. Lorson had already done on SMARD. We were impressed by how much of a handle they already had on the disease. They were ahead of the game. That was great news for us on the family side; at the time, we were aware of only one other lab in the country — the Jackson Lab in Maine — doing work in this area. We couldn’t believe that, wow, there’s a second lab and they are already in gear, they already have a lot of good things going.
“Then, Lisa got me in the loop with Monir, and I talked to her a few times,” Sims continues. “They were having a funding issue, which is not surprising because of how rare the disease is. When we first learned about the work being done at the Jackson Lab, my in-laws agreed to fund SMARD research at Jackson. After learning what Dr. Shababi and Dr. Lorson were doing, I talked to my in-laws again and asked if they would be interested in funding Monir’s research. My father-in-law and I had a few conversations with Monir and Chris Lorson, and then my in-laws decided to do another fund, this time at Missouri, that started this past December.”
*****
“If you look back a number of years, there has been a gene therapy on the translational side that has had exceptionally powerful results in SMA,” says Lorson. “AveXis now has a Phase 2 clinical trial going for their gene therapy product, which has the potential to be very impactful. It has demonstrated efficacy in SMA, but also provides an important proof of principle for gene therapy as a whole. So, it was really exciting to know that there’s only one gene responsible for each of these horribly devastating diseases, SMA and SMARD. It allows you to consider following a similar path. Knowing that, Monir started developing a project that was gene therapy, gene replacement for SMARD.
“Whenever I talk about this, I give about 110 percent of the credit to Monir,” Lorson explains. “Monir has really been the driver of this entire project. Originally, I said, ‘Monir, I’d really like you to develop this gene therapy for SMARD, I think it’s a really exciting area of research. I’ll check back in about six months.’ When I did, we had the mice, we had the vector and she was doing the experiments. That’s exactly the kind of gumption that you hope to find. She did all of that. My role was to say, ‘Good job, Monir!’
“She was the first author on an important paper in Molecular Therapy published in 2016,” Lorson continues. “Based upon that, and the level of excitement, people found her. Through Facebook and Facebook friends, they started to communicate back and forth. Monir is driving it. Monir is doing it.
“AAV9 is in clinic for a number of other diseases, but every time you put a new gene in, you have to go through the Food and Drug Administration,” Lorson says. “That’s why the process isn’t as simple as it might appear to be. Every single time you change that vector — that gene delivery vehicle — you have to get it approved.”
*****
“My in-laws have been very generous, but you need a lot of capital to do this research,” Jill Sims says. “SMARD is so rare that progress will probably come only from academic research. You really need a lot of support and you need a lot of funding from various sources. Right now, our life continues the same. It’s great that everybody is doing this great research, but you need so much more for a cure. That’s what everybody wants; we want our kids to be normal.
“A day in the life of someone with SMARD is very difficult,” Sims says. “There’s a lot that has to be done to have a normal life, and there are a lot of obstacles to that, so you’re constantly trying to overcome those.
“This disease is devastating,” Sims continues. “It can take away every basic human function: the ability to sit, crawl, stand, walk, talk, swallow, feed oneself, clean oneself, use writing utensils and so on. The disease also makes the person more likely to have respiratory problems since they can’t breathe or even cough on their own. It is hard as a parent. Every day we live with the potential fatality of this disease. If their trach tubes come out, they cannot breathe. These trachs sit in their windpipes, held in by ties, like a tight necklace. It is not secure.
“You may go months without anything happening then, all of a sudden, it’s coming out. When that happens, she may only have 60 or so seconds to live,” Sims says. ”You have to have someone always watching them, either a specially trained nurse or a parent, who is a trained caregiver.
“That’s the hard part that we always live with,” says Sims. “Yes, she looks good, and she goes to school, and she’s in activities, to some degree. We adapt everything so she can do as much as possible. But, she is living with a fatal disease that is non-treatable. We basically just manage her symptoms. We know very well that we could lose a second child. That’s what is hardest on us. Even though there are these great advances, she is alive because of amazing machines. Every day presents the chance that she could die.
“When we take Catherine places, there are always at least 10 machines that go with her,” Sims says. “Everything just takes longer. We have a special van with a lift, because she’s in a wheelchair. You are in the thick of trying to make what is not normal to be normal.
“You can’t just pick up your child and go, you can’t feed them a different way, or put a different outfit on them,” Sims continues. “Those are the silly things I took for granted having had a healthy child before. I just did her hair, brushed her teeth, and put her in whatever, and fed her whatever I wanted. Catherine cannot do that. It’s the small things that you take for granted, and there are so many ‘small’ things. We are fortunate to have excellent in-home nursing care, but this also means that my husband and I have had to sacrifice a lot of our privacy. And, I’ve had to give up a lot of my mothering, because I have someone else that always needs to know what I’m doing. That’s hard.
“So, we want a cure,” Sims states. “We are all in. We are always fighting the disease. Our goal would be to have a cure as fast as possible, because the older the kids get, the less chance you have of curing them. This is a neurologic disease; it is hard to get those nerves back. We realize that our kids may be too old. Catherine will be 5; Lisa’s Silas is 8 or 9. They’re kind of old. The ideal time would be right at birth or shortly thereafter. So, that’s what we want. We want the big places — the big funding sources — to realize how important this is, even though it affects only a small number of people.”
*****
“Our gene therapy vector is a very powerful tool,” Lorson says. “It is early days, in terms of trying to push it to the clinic, but we’re trying to do all the important pre-clinical questions.
“There are a number of questions you have to ask,” Lorson continues. “When do you deliver that kind of vector? Does it work only if you do it right at birth, before disease develops? Can you correct the disease, in other words, once the research animals have the disease, can you bring them back to more of a normal state? Or, once that happens, is it just too late for something like gene therapy? We want to deliver what they want to see, in terms of working hard and getting results out. That is what we are trying to do.
“I want to say, ‘Thank you,’ in the biggest way possible to the Sims family,” Lorson says. “Their generosity is really amazing. We consider this an exceptional honor. We want to be the best stewards they could possibly find, of their trust and of their funds. People go out and raise these funds — in some cases, through car washes and bake sales — so you have to put a particularly high value on those dollars. My fondest hope is that we do that every day.”
If you would like to help in the battle against diseases that could someday be relieved through gene therapy, please visit this page.
Gene therapy treating the neurodegenerative disease, SMARD1, shows promising results in mice studies.
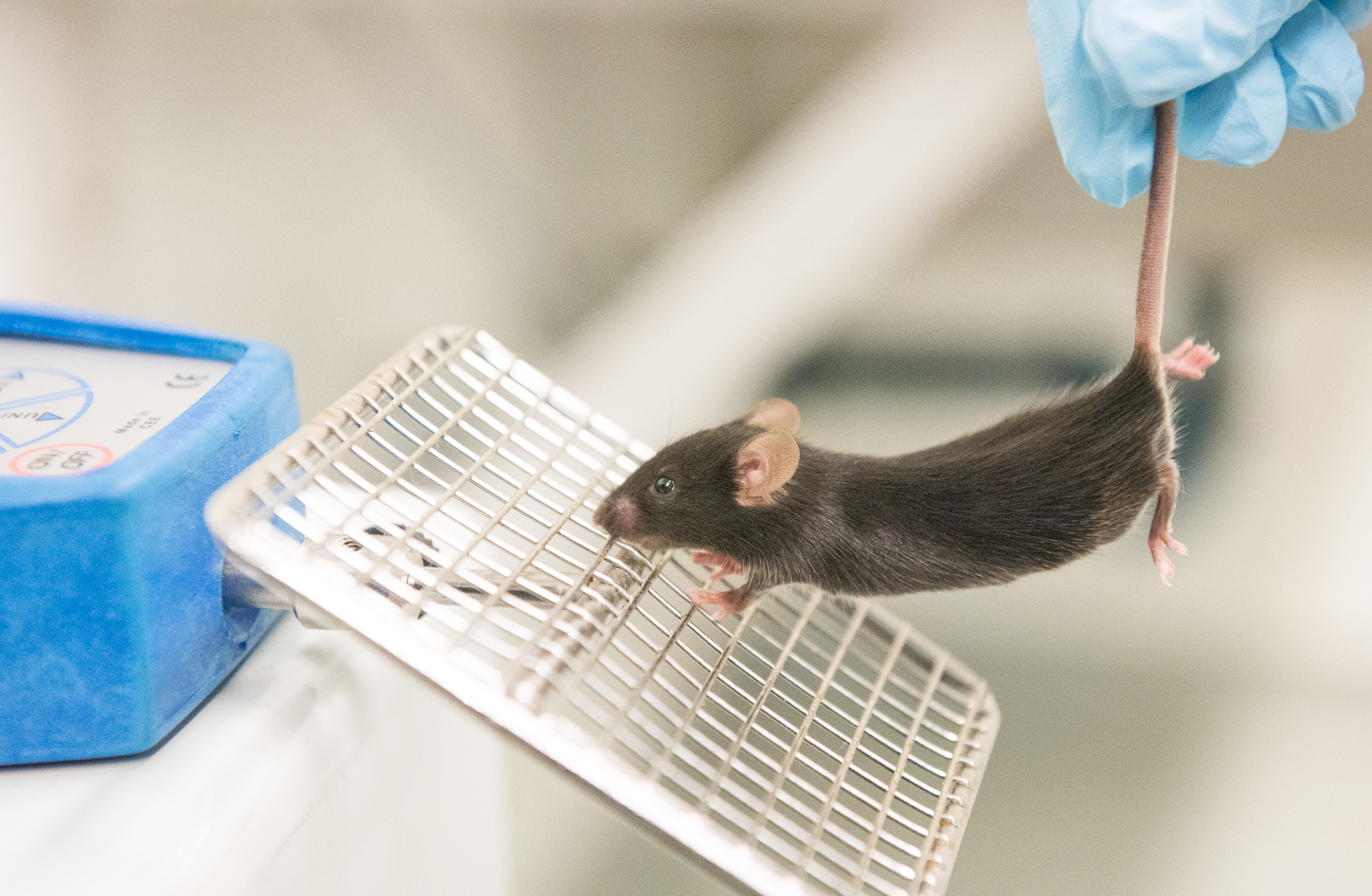
Shababi uses an instrument to measure grip strength in the forelimbs of mice. Healthy mice are able to cling on with a stronger grip than SMARD1 mice. | photo by Jennifer Lu, Bond LSC
Monir Shababi was confident her experiments treating a rare genetic disease would yield positive results before she even ran them.
Scientists had success with a similar degenerative neuromuscular disease, so she had every expectation their strategy would work just as well in her mice.
Monir Shababi, an assistant research professor in the Department of Veterinary Pathobiology, studies SMARD1 in mice. | photo courtesy of the Department of Veterinary Pathobiology
“I was expecting to get the same results,” said Shababi, an assistant research profession in Christian Lorson’s lab at the University of Missouri Bond Life Sciences Center. Shababi studies spinal muscular atrophy with respiratory disease type 1, or SMARD1.
The treatment worked, but not without a few surprises.
Her findings, published in Molecular Therapy, a journal by Nature Publishing Group, are one of the first to show how gene therapy can effectively reverse SMARD1 symptoms in mice.
In patients, SMARD1 is considered such a rare genetic disorder by the U.S. National Library of Medicine that no one knows how frequently the disease occurs. It’s only when babies develop the first symptom—trouble breathing–that pediatricians screen for SMARD1.
Shortly after diagnosis, muscle weakness appears in the hands and feet before spreading inwards to the rest of the body. The average life expectancy for a child diagnosed with SMARD1 is 13 months. There is currently no effective treatment.
Since the neuromuscular disease is caused by a recessive gene, SMARD1 comes as a shock to the parents, who are carriers but do not show signs of the illness, Shababi said. This genetic defect prevents cells from making a particular protein that scientists suspect is vital to replication and protein production.
The hereditary nature of the disease has a silver lining, though. Because SMARD1 is a caused by a single pair of faulty genes and not multiple ones, it is a prime candidate for gene therapy that could restore the missing protein and reverse the disease.
To do that, Shababi set up a dose-response study using a tiny virus to carry the genetic instructions for making the missing protein. She injected newborn mice with a low dose of the virus, a high dose, or a placebo with no virus at all.
Injecting at different doses allowed her to ask which dose worked better, Shababi said.
According to the previous research, a higher dose should have resulted in a more effective treatment.
“So I thought a higher dose was going to work better,” Shababi said.
Instead, the high dose had a toxic effect. Mice given more of the virus died sooner than untreated mice. Meanwhile, mice given a low dose of the gene therapy lived longest. They regained muscle function and strength in both the forearms and the hind limbs and became more active.
In fact, some of them survived long enough to mate and produce offspring.
Initially, Shababi housed her SMARD1 mice in the same cage as their mothers so that the moms could intervene if the sick pups become too feeble to feed themselves. When the male pups became well, their moms became pregnant.
“That was another surprise,” Shababi said. “That was when I knew I had to separate them.”
Shababi marks a pup, only a few days old, with permanent marker so each mouse in her study can be identified. | photo by Jennifer Lu, Bond LSC .
In another twist, Shababi discovered that the route of injection also mattered.
To get the treatment across the blood-brain barrier and to the spinal cord, Shababi used a special type of injection that passes through the skull and the ventricles of the brain, and into the spine.
This was no easy task.
The newborn mice were no larger than a gummy bear. To perform the delicate work, Shababi — who has written a chapter in a gene delivery textbook about this procedure — had to craft special needles with tips fine enough for this injection. She added food coloring to the injection solution so she could tell when it had reached its intended destination.
“After half an hour, you will see it in the spinal cord,” Shababi said. “The blue line in the spine: that’s how you can monitor the accuracy of the injection.”
Unfortunately, repeated injections in the mice caused hydrocephaly, or swelling in the brain.
“They get a dome-shaped head,” Shababi explained.
The swelling happened in all three treatment groups, but most frequently in the group that received a high dose of viral gene therapy. This reinforced the finding that while a low dose was beneficial, a high dose was even more harmful than no treatment at all. It’s unclear why.
Christian Lorson is a professor of veterinary pathobiology at the Bond LSC. His research focuses on spinal muscular atrophy and more recently, SMARD1. | photo by Hannah Baldwin, Bond LSC .
The Lorson lab plans to continue studying SMARD1 and this treatment, in particular, how changing the delivery routes for gene therapy can improve outcomes in treating SMARD1.
“It’s not as simple as replacing the gene,” Lorson said. “It comes down to the delivery.”
Injections in the brains of mice are meant to mimic spinal cord injections in humans, but intravenous delivery could be another option. However, intravenous injections, which travel through the blood stream and to the entire body, might cause off-target effects that could interfere with the effectiveness of the treatment.
Once researchers better understand how to optimize dosing and delivery on the cellular and organismal level, the therapy can move closer to clinical trials, Lorson said.
Even though gene therapy for SMARD1 is still in its early stages, he said he was optimistic that developing treatments for rare genetic diseases is no longer the impossible task it seemed even ten years ago.
Spinal muscular atrophy (SMA) is a prime example of a recent success, Lorson pointed out. In the last six years, gene therapy for that disease has moved from the research lab to Phase I clinical trials.
“While it feels like a long time for any patient and their families,” Lorson reassured, “things are moving at a breakneck pace.”
The study, “Rescue of a Mouse Model of Spinal Muscular Atrophy With Respiratory Distress Type 1 by AAV9-IGHMBP2 Is Dose Dependent,” was published in Molecular Therapy, a journal published by Nature Publishing Group. This work was supported by a MU Research Board Grant (C.L.L.); MU College of Veterinary Medicine Faculty Research Grant (M.S.); the SMA Foundation (C.P.K.); National Institute of Health/National Institute of Neurological Disorders and Stroke grants; and the Missouri Spinal Cord Injury Research Program (M.L.G.).